Your cart is currently empty!

CASE REPORT
Primary root canal treatment of tooth 44 presenting with an apical split.
We present a case of primary endodontic treatment of tooth 44 presenting with split in the apical one third. This clinical case highlights the importance of precise preliminary diagnosis, careful planning of the endodontic access, and adapting the therapeutic approach to the individual anatomy of the root canal system.
The patient presented to our clinic with pain localized on the right side of the mandible. The pain was triggered and intensified by thermal stimuli and was more pronounced at night. The nature of the pain was suggestive of an inflammatory process involving the pulp, requiring a detailed clinical and radiographic assessment.
During the clinical examination, a carious lesion was identified in the cervical region of tooth 44. The lesion was located in an area that posed specific challenges in terms of access, as well as subsequent isolation and restoration of the tooth. (Fig. 1)

Fig. 1
The patient presented to our clinic with a pre-existing CBCT scan, which revealed the close proximity of the carious lesion to the pulp chamber, as well as the presence of an apical split within the root canal system. The three-dimensional imaging was essential for preliminary planning, as it enabled assessment of the anatomical complexity and helped anticipate the need for careful mechanical preparation of the canal ramifications. (Fig. 2)

Fig. 2
Diagnosis:
Pulpal diagnosis: symptomatic irreversible pulpitis
Apical diagnosis: normal apical tissues
Based on the clinical symptoms, radiographic findings, and the established close proximity of the carious lesion to the pulp chamber, the decision was made to proceed with endodontic therapy.
Following administration of local anaesthesia, caries excavation was initiated. During removal of the carious tissue, communication with the pulp was established, confirming the need for endodontic treatment. The cervical access allowed easy localisation and preparation of the lingual canal branch. However, due to the risk of instrument separation when attempting to prepare the buccal canal through the cervical cavity, the decision was made to create an occlusal endodontic access.
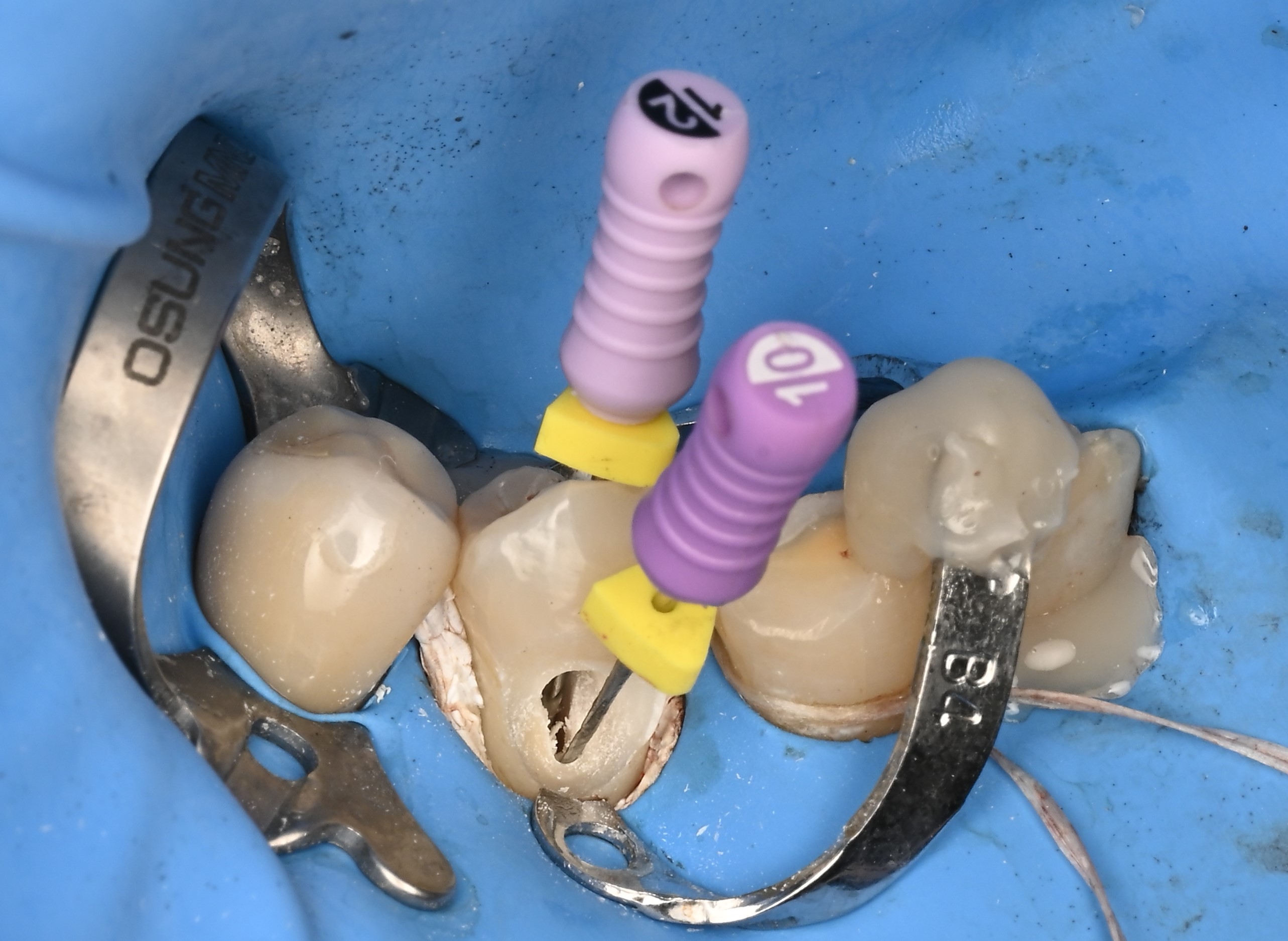
Fig. 3
The occlusal access facilitated preparation of the root canal system and provided a more direct and safer pathway to the buccal canal branch. This modification of the access cavity was important in reducing mechanical stress on the instruments and allowing better control during canal preparation. (Fig. 4)
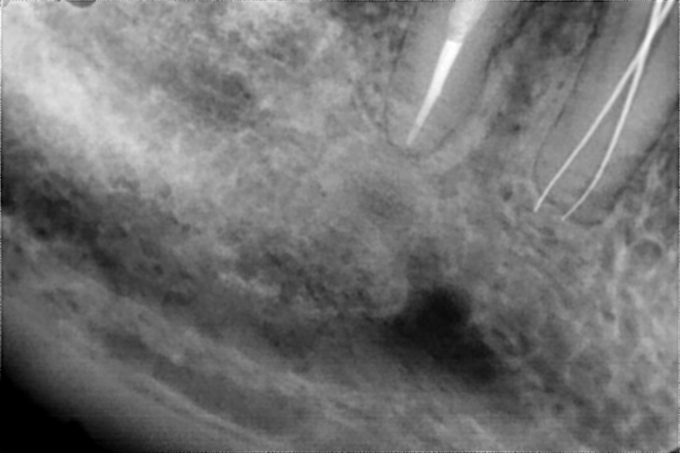
Fig. 4
In this case, to improve access during treatment, the decision was made to place rubber dam isolation extending from tooth 45 to tooth 42. A No. 2 Osung clamp was used as the master clamp, while a B4 Coltene clamp was used as an auxiliary clamp to provide improved soft tissue retraction and better buccal access to tooth 44. (Fig. 5)

Fig.5
For additional stability, the auxiliary clamp was secured to the adjacent tooth using flowable composite, and Teflon tape was placed in the cervical area to provide further retraction and isolation of the operative field. This isolation strategy ensured a dry working field, improved visibility, and better control of the operative area, which is particularly important in cases involving cervically located lesions and complex canal anatomy.
For the mechanical preparation of the canals, we used the Super System Advanced kit, which allowed for conservative preparation of the root canal system. The approach was aimed at preserving as much sound tooth structure as possible while ensuring adequate preparation of both canals. The final canal preparation corresponded to size 25.04.
The tooth was obturated using a bioceramic sealer (Avalon Biomed) and calibrated gutta-percha points size 20.04. The choice of a bioceramic sealer was based on the need for good adaptation to the canal walls and reliable sealing of the complex apical anatomy.
During obturation, the main challenge was the ability to place both gutta-percha points simultaneously without interference, while ensuring that each point reached the working length. This required careful try-in, control, and adaptation of the points in order to achieve predictable obturation of both branches of the root canal system. (Fig. 6) Placement of the gutta-percha points was possible entirely through the cervical access, which facilitated obturation of the root canal system and allowed both branches to be filled simultaneously.
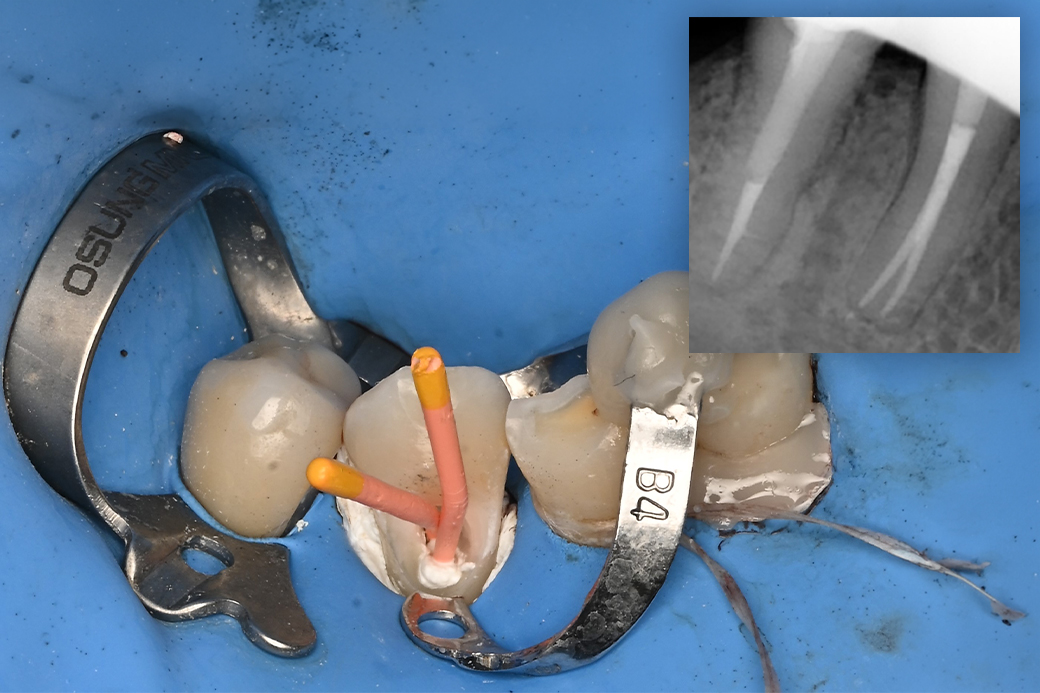
Fig. 6
The tooth was restored with composite resin. To provide additional reinforcement, a fibre-reinforced composite, everX Flow Bulk, was used in the core. This approach aimed to strengthen the remaining tooth structure. (Fig. 7)

Fig. 7
The patient was referred back to his treating dentist, as prosthetic treatment was planned.
Conclusion
The presented clinical case demonstrates the importance of CBCT diagnostics in the presence of anatomical variations within the root canal system. The apical split of tooth 44 required modified endodontic access, careful isolatio
Author: Dr Konstantin Kostadinov
Affiliation: Dentaprime Academy



